Duodenal Stricture
This work is licensed under the Creative Commons Attribution-Noncommercial-No Derivative Works 3.0 United States License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/3.0/us/ or send a letter to Creative Commons, 171 Second Street, Suite 300, San Francisco, California, 94105, USA.
Publication Date: 2007-01-27
History
1 Year old male castrated Great Dane. 1 week history of inappetance and vomiting. Surgery for foreign body and intessusception performed one week ago.
1/23/06- Presented to VMTH Emergency Service for a distended abdomen, one week following surgery for a foreign body/intussusception performed by the rDVM. Septic peritonitis was diagnosed and Duke was immediately taken to surgery. Exploratory laparotomy revealed marked omental adhesions and multiple perforations throughout the jejunum. 60cm of the jejunum were resected, a prophylactic gastropexy was performed, and abdominal drains were placed. He also has a history of HOD for which he had been receiving prednisone (10mg PO SID). Rx post op: Clavamox 375mg PO BID, famotidine 10mg PO BID, tramadol 50mg PO BID. Doxycycline: 1 1/2 tabs BID.
9/28/06 for 1wk Hx of inappetence and acute onset V.History of intestinal surgery one week previously. Had a foreign body and intessusception with septic peritonitis and multiple adhesions. Several perferations were present. 60 cm of the jejunum was resected, and prophylactic gastropexy was performed.
Findings
The pyloric portion of the stomach and the proximal duodenum are dilated with fluid and gas. The duodenum travels dorsally on both lateral projections, which is typical of dogs who have had a gastropexy performed. The duodenum narrows abruptly just ventral to L2.
Diagnosis
Duodenal-jejunal stricture at the site of previous resection and anastomosis.
Discussion
This case is unusual because the small intestinal obstruction is a complication of previous surgery. The signs are similar to a high obstruction though, with an enlarged stomach and duodenum, and more normal sized jejunum.
We were fortunate to have gas acting as a natural contrast medium and outlining the stricture on both lateral projections. Otherwise, barium would have been an appropriate next step. Ultrasound was also performed, but this is a difficult diagnosis to make with ultrasonography.
3 images
Additional Images

The ultrasound in this case was very challenging. It's difficult to access the proximal duodenum in a deep chested dog like a Great Dane, and the altered anatomy from the gastropexy made things difficult to find.
This image demonstrates the dilated portion of proximal duodenum as it narrows down at the stricture site. The arrows define the bowel walls cranial and caudal to the stricture.
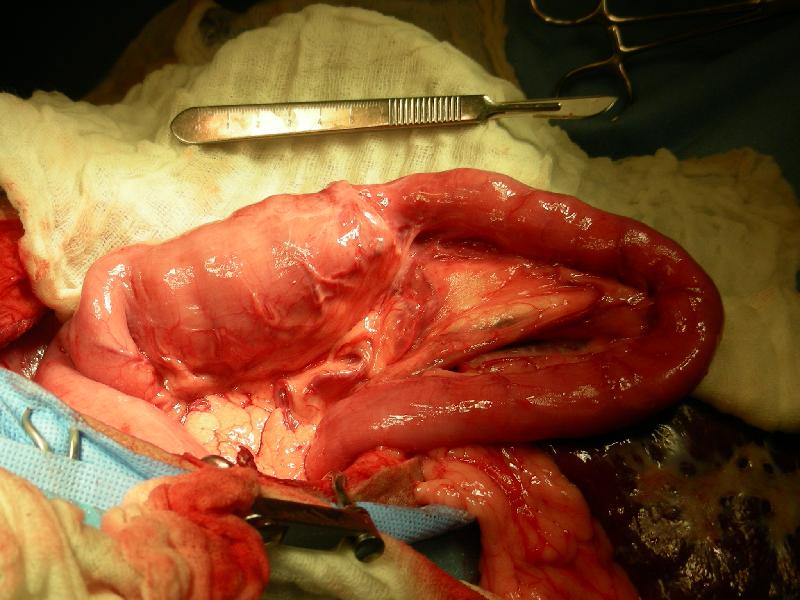
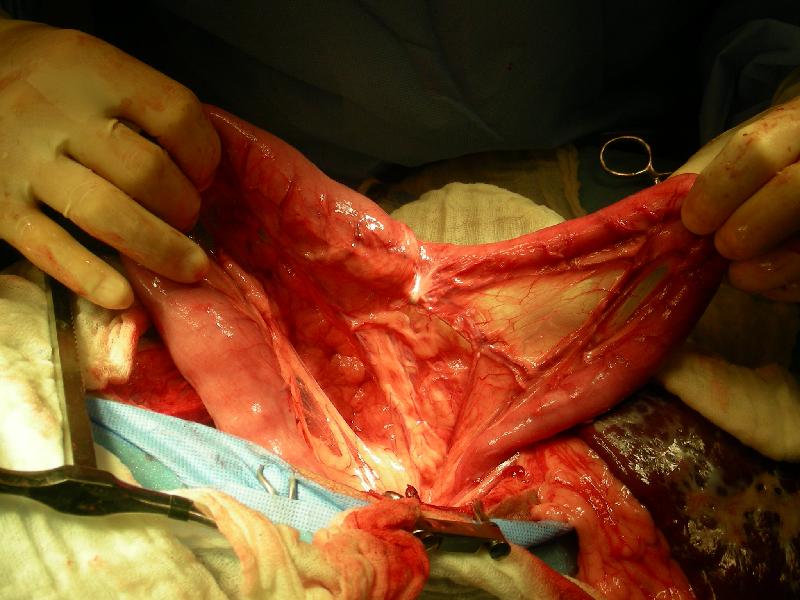
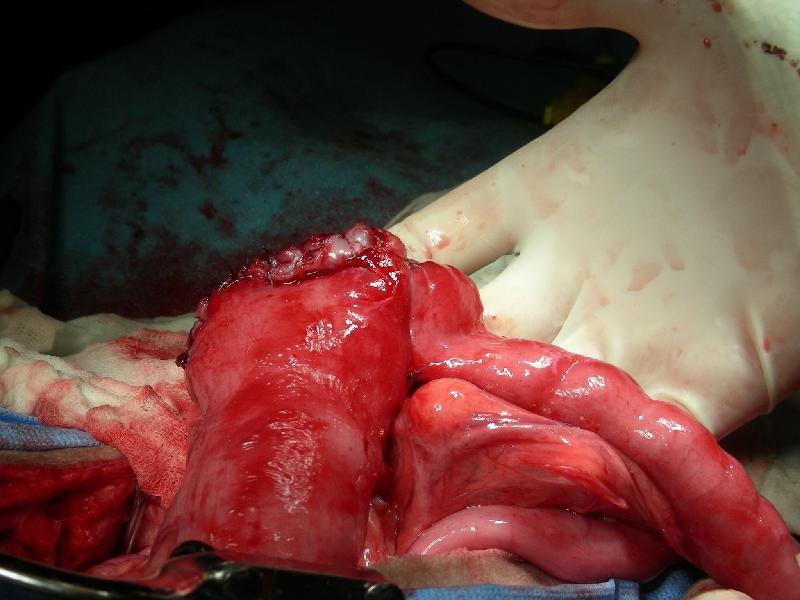

Surgery report
Description of Surgical Procedures: The patient was placed in dorsal recumbency, clipped and aseptically prepared. A ventral midline incision was made through skin and subcutaneous tissue from the xiphoid caudally to approximately 5cm cranial to the prepuce using a #10 blade. The linea was incised with a #15 blade and the incision extended with Mayo scissors. White streaks were noted on the capsule of the spleen and on the surface of the left medial liver lobe. Omental adhesions were noted throughout the abdomen. The duodenum was dilated at 5 cm, and acutely narrowed to 2.5 at the duodeno-jejunal junction (previous anastomosis site). Prolene suture material was visible through the scar tissue at the site. The intestine was hypermotile in this region. The vessels in the mesentery were isolated and ligated using 3-0 PDS. The region of the duodeno-jejunal junction containing the stricture was resected and a functional end to end anastomosis was performed using a GIA 50 stapler and a TA 55 stapler. The end was oversewn with 3-0 PDS in an simple continuous pattern. A 1 cm region of TA staples were noted to be separated from the opposite side, and the region was closed with 3-0 PDS in a simple interrupted pattern. An omental patch was placed over the resection and anastomosis site and held in place with a single 3-0 PDS interrupted suture. The abdomen was lavaged with sterile saline. The linea was closed with 0-PDS in a continuous pattern. The subcutaneous and subcuticular layers were closed using 3-0 monocryl in a simple continuous pattern. The skin was opposed with staples. The resected intestine was submitted for histopathology.